


Avvanzo P.¹, Ciavarella D.¹, Avvanzo A.², Giannone N.¹, Carella M.1, Lo Muzio L.¹ ¹
Department of Oral Surgery and Oral Pathology, University of Foggia, Dean: Prof. L. Lo Muzio. ² Private Practitioner, Foggia, Rome.
Abstract
The immediate placement of dental implants in aesthetic areas is a primary challenge for modern implantology. The underlying treatment goal is to preserve the natural periodontal architecture; in recent years, concurrent goal has also been to reduce the period between implant placement in the fresh extraction socket and delivery of the definitive restoration, but adequate long-term data are still lacking on the efficacy of this technique. A 3- to 5 year retrospective analysis of 282 dental implants immediately placed into extraction sockets, and temporized with non-occluding provisional prostheses, has been undertaken. All recorded outcomes, complications and a proposed protocol for management of immediate function are discussed.
Introduction
Placement of dental implants for the restoration of missing teeth is a well-established treatment option. According to conventional protocol, implant placement should be delayed up to one year after tooth extraction to allow for complete alveolar bone healing 1. After implant placement, conventional protocol recommends a load-free period of 3-6 months to ensure osseintegration of the implants. Such a long treatment period was an obvious drawback to patient acceptance of this treatment modality. The conventional protocol has been challenged in recent decades by reducing the time between the extraction of a tooth and the placing and loading of the implant. Various classifications have been suggested for the timing between tooth extraction and implant placement. This can make it difficult to compare the outcomes of previous studies. In a recent systematic review 2 of the dental literature, an implant placed in a fresh extraction socket was denoted an immediate implant. An implant placed in an extraction socket within 8 weeks after tooth extraction was called immediate-delayed and implants placed later were called delayed implants. Apart from reducing the time period and the number of surgical interventions, other advantages of immediate or early (immediate-delayed) implant placement in the extraction socket have been suggested. These include better implant survival rates, improved aesthetics, maintenance of the hard and soft tissues at the extraction site, and higher patient satisfaction compared with delayed implant placement 3,4,5 The success rates of new surgical techniques and new materials today help to make clinicians more confident in proposing prosthetic rehabilitation with implants, but long-term data are still generally lacking to adequately support evidence-based treatment planning. This article reports on a 3- to 5-year retrospective analysis of 282 immediately placed and immediately temporized dental implants.
Materials and Methods
A chart review was conducted of 231 patients who had been treated for immediate single tooth rehabilitation. The authors wanted to verify if there was a difference in results using different implant morphologies in fresh extraction sockets followed by immediate temporization and early loading. The inclusion criteria for implant placement included unsalvageable anterior teeth (Fig. 1a), and adequate residual apical bone below the tooth ≥ 4 mm. Additional exclusion criteria included, smokers, severe bruxism and/or clenching habits, previous history of failed implants, untreated periodontitis, the inability to achieve primary implant stability, and the need for bone grafting. Periapical (Fig 1b), panoramic radiographs and cross-sectional tomographs were used to initially evaluate the bone quantity and the quality of the implant recipient site and to determine the length of the implant required. Anamnesis and radiographic data were collected before operating. All patients underwent preliminary comprehensive dental care. Written patient consent was obtained before proceeding.
On the day of surgery, 2 gr. amoxicillin + clavulanic acid solution were given one hour before surgery. Lornoxicam 8 mg. was given as analgesic only when required. In addition, patients rinsed with a 0.2% chlorhexidine digluconate solution for 1 min. Local anesthesia was achieved with 2% Mepivacaine solution. Tooth extraction was performed using surgical blades to incise the periodontal ligament and preserve the periodontal architecture and minimize trauma (Figs.1c-2b). The tooth was gently removed minimizing damage to the alveolar housing and the root was extracted with light twisting movements to avoid breaking of any bony margins of the alveolus. Granulation tissue, if present, was carefully curetted and removed. The alveolar socket was irrigated using sterile saline solution. All osteotomy preparations were made with the aid of a surgical guide. The implant site preparation was initiated with a small pilot bur (diameter 1.2 mm.) to help establish proper drill orientation. The pilot bur was angled palatally or lingually to help preserve the buccal wall of alveolar bone. Implants were placed 2-4 mm below the crest of the ridge and below the apices of the adjacent tooth roots. Implants were selected for maximum use of available bone. Abutment angles were limited to not more than 15° and implant necks bore sufficiently hard and soft tissues. Abutment for 2P2S implants were shorter than usual in order to avoid a vertical cantilever effect and be sure of the resistance of bone to no axial forces. After implant placement (Fig. 1c), abutments were attached and provisionally restored with crowns (Fig. 1d). Absolute lack of occlusal and lateral contacts was verified using articulating gloss paper. In all those cases presenting altered gingival contours aspect, sutures were placed to improve aesthetics. Patients were provided with post-operative instructions and dismissed. Follow-up was scheduled weekly for two months until the final prosthetic phase. After delivery of the definitive restoration, patients were recalled every 6 months for the next 5 years. Additional cases are illustrated in Figures 2a-d and 3a-d.
Results
Different designs of implants were included in the analysis: 152 (53.90%) two-piece cylindric two-stage implants (2P2S)(internal hexagonal connection), 34 (12.05%) two-piece, one-stage screw-type transgingival implants (2P1S) (abutment conical connection), 96 (30.04%) one-piece, one-stage, screw-type implants (1P1S)(Fig.4). Diameters ranged from 3.4 mm. to 6.0 mm. Lengths ranged from 11.5mm. to 14.5mm. The replaced teeth were in anterior maxillas (93 incisors, 38 canines) and mandibles (57 incisors, 9 canines) and lateral regions (64 maxillary premolars, 21 mandibular premolars). Mean patient age was 34.3 years (range = 20-57 years). The mean interval time between implant placement and definitive restoration was 24 days (range =7-43 days). During this period, the abutments were provisionally restored with single-tooth restorations so that the soft tissues could heal in the desired anatomical contours. Care was taken to avoid traumatic occlusal or lateral contact with other teeth. No post-surgery edema was reported. Pain was light and analgesics were only used in a few cases. 18 of 282 implants (6.38%) failed before loading; there were no failures after delivery of the final prostheses. Among the failures, 10 (3.54%) implants had been placed in poor density bone; in 4 of these cases failure occurred secondary to fracture or loosening of the connecting internal screws. The other 8 (2.83%) implants failed secondary to infection. From 3 to 5 years after surgery, all other implants have remained fully functional and maintained aesthetic efficiency. Papilla and marginal bone peaks have been preserved or improved. Occasionally 2P2S implants showed loosening of the abutment connecting screws which needed to be tightened. This problem was especially common to second premolars and canines replaced by abutments attached to screw-type implant systems. Full-contour, solid abutments, screwed directly into 2P1S implants, did not show the setbacks of former implants (Fig. 4): the problem found with this kind of implant was that they showed weaker primary stability due to their poor thread engagement. For this reason, they were used in a few cases with very good bone quality. In fully osseointegrated implants, there were 22 cases of screw loosening for 2P2S implants, 1 case of abutment loosening for 2P1S implants, no problems with 1P1S implants. The rates, indicating failures and non-failures related adverse events for each kind of implant, were 20.6% for 2P2S implants, 17.6% for 2P1S implants and 4.1% for 1P1S implants. This analysis was performed to determine which system was the least problematic and easiest to manage.
Figure 4

One of the most emphasized features of the conventional protocol was the requirement for a submerged healing period free of functional stresses for a period of 3 to 6 months6,7,8. During this time, patients were obliged to wear total or partial removable prostheses for provisional esthetics, phonetics and chewing function9. The ability to diminish the interval between surgical and prosthetic phases reduces discomfort for patients. That is why clinical attention has been increasingly focusing on immediate loading10,11,12,13,14,15. As for achieving good primary stability and osseointegration in immediately loaded implants, the success rate of the technique has been confirmed by histologic samples from animals and humans16,17,18. Prosthodontic techniques to enhance soft tissue contour by using custom abutments and provisional crowns to support the peri-implant mucosa during healing have been described in case reports and retrospective and prospective cohort studies 18,20. It was concluded that immediate or immediate-delayed placement of implants is a viable treatment option and may be associated with better outcomes in terms of esthetics and patient satisfaction compared with conventionally placed implants21,22.
The theoretical and clinical basis of immediate loading deals with two considerations: the success rate of non-submerged one-stage implants, reported in the dental literature, and the opportunity to use immediate loading as a means of osteogenetic induction during bone healing23. According to Branemark 24,1,6 connective tissue healing via a submerged surgical technique was a primary condition for osseointegration, allowing a connective-epithelial seal to protect the implant from contamination. The evidence25,26,27,28,29,30 of non-submerged implant success has invalidated this principle. According to Carter and Frost31,32,33 and Wolff’s law, bone undergoes a variable deformation when subjected to a variable load applied. This deformation leads to an increase of bone remodelling for values between 2000 and 4000 μstrain (the physiological range of bone deformation under loading). Over these values, bone resorption is possible. For this reason every deforming load should be avoided or re-directed to other teeth during healing time so that the old paradigm “no load on implants during healing time” becomes “no movement of implants”.
Regarding the presence or absence of contacts in occlusion, a distinction has to be made between immediate loading and immediate function34. Absence of contact points does not mean absence of load: food incision by implants replacing incisors and forces generated by tongue or orbicular lip muscles cannot be avoided. Therefore, even if there is no centric occlusal contact among jaws, which appears only during swallowing35, provisional crowns on implants are, nevertheless, stressed by chewing cycles. In a multiple-implant system, the prosthetic structures impose a rigid splint to the implants and break up chewing forces into different vectors with no dangerous intensities and directions. In single implant cases, the situation is very different: a single implant works in the same background of teeth and undergoes the same forces. A totally edentulous patient, who undergoes multiple implant system rehabilitation, develops weaker force than a partially edentulous patient with one or more missing teeth.
For immediate placement and loading of implants, another parameter has to be considered: alveolar bone resorption after extraction. Often immediate replacement is required in upper incisors because of their highly esthetic value. The real enemy for integration is not immediate function but micro-movement at implant-bone surface36. The threshold of permitted movement is between 50 and 100 μ37,38. Leaving out macro- and micro-retention features, by which self-threading implants and micro-rough surfaces are the gold standard26, other success factors include a sufficient number and optimal positioning of implants, good quality and quantity of bone, passive fit of prosthetic structure at metal-metal interface and rigid mechanical tolerance on implants7 and occlusal pattern. These parameters all pertain to multiple implant systems.
This study is not a randomized clinical trial but a retrospective analysis of consecutive cases, which is an important first step for developing evidence-based data34. In the Cochrane database, only two controlled clinical trials exist concerning with immediate loading, and both deal with immediately loaded multiple implants systems in mandible2. These two studies conclude that, in the mandible, immediate loading is possible, but not surely predictable. No clinical trial exists in the Cochrane database as immediately placed and loaded implants.
Bone undergoes approximately 23% resorption in the first 6 months after extraction and an additional 11% during the next 2 years39. These data underscore the importance a comprehensive treatment plan to optimize available bone volume, reduce patient discomfort and improve aesthetics and function.
This study found that the best results were achieved using 1P1S implants; this choice improved esthetics and eliminated prosthetic setbacks associated with loosening of connecting screws. The 1P1S implants were treated as if they were teeth, prepared for appropriate angles and emergence profiles and then restored with cemented crowns.
The protocol, presented below, can make a difference in achieving full aesthetic and functional results, minimize problems for patients and reduce treatment time. The protocol used in the present analysis can be summarized as follows:
- bi- or tri-cortical implant-bone contact.
- appropriate implant length and diameter.
- primary stability.
- major implant deepening.
- palatal or lingual direction of placement.
- functional loading.
- no occlusal or lateral contact during provisional phase.
Conclusion
Within the limitations of this retrospective analysis, immediate or early placement of implants was a viable alternative to delayed placement. Long-term randomized prospective data are needed to correctly evaluate the equivalence between this protocol and the conventional delayed approach.
Photos
Fig.1a Non-salvageable lateral upper incisor.
Fig.1b X-ray showing reconstruction and infection at apex.
Fig.1c Extraction performed with maximum respect for soft tissues and bone. A 1P1S implant is placed.
Fig.1d A provisional crown has been delivered to the abutment. The entire zone has been washed.

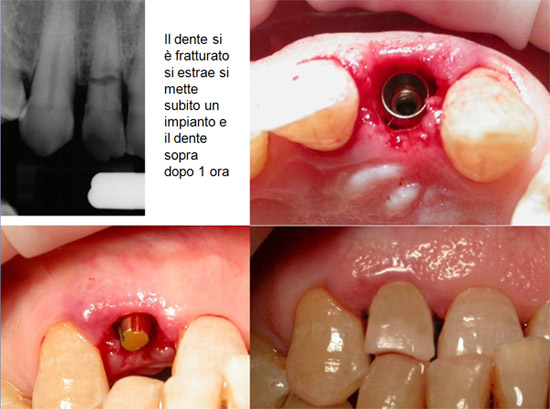
Fig.2a Fractured maxillary lateral incisor. Conventional treatment was rejected.
Fig.2b Extraction and placement of a 2P1S implant.
Fig.2c A conic abutment shorter than usual has been attached to the implant.
Fig.2d A provisional crown was delivered with tooth-like occluding contact.

Fig.3a Unsalvageable lateral incisor root.
Fig.3b Soft and hard tissues remained intact during extraction.
Fig.3c palatal placement of a 2P1S implant.
Fig.3d Provisional crown in place.


Dentista Campania, Napoli
Vedi la scheda
Dentista Toscana, Pistoia
Vedi la scheda
Dentista Liguria, Savona
Vedi la scheda
Dentista Sicilia, Ragusa
Vedi la scheda
Dentista Toscana, Lucca
Vedi la scheda